
DOI: 10.5281/zenodo.21072411 · UDC: 616.61-036.12-06:[616.98:578.834.1]
Objectives. Chronic kidney disease and COVID-19 have a bidirectional interaction: on one hand, it increases the risk of severe COVID-19, while SARS-CoV-2 may accelerate renal deterioration in vulnerable patients. We aimed to assess medium-term renal status after COVID-19 and to identify independent unfavorable prognostic factors for chronic kidney disease progression using multivariate regression models.
Methods. In a prospective cohort study, 280 pre-dialysis patients (KDIGO stages G1–G5) were evaluated in a tertiary nephrology center. Participants were allocated to two matched groups: post-COVID-19 patients with chronic kidney disease (n=140) and non-COVID control patients with chronic kidney disease (n=140), comparable for age, sex, disease stage, and major comorbidities. Clinical variables, renal and metabolic parameters (including proteinuria, phosphate, and hemoglobin), inflammatory markers, and SF-36 quality-of-life scores were collected at follow-up. Group comparisons, correlation analyses, and multivariate logistic regression were performed. Advanced chronic kidney disease was defined as stage G4–G5 at follow-up.
Results. Post-COVID and control groups showed similar renal function at follow-up (mean eGFR ≈35 mL/min/1.73m2; p>0.5), with no significant differences in serum creatinine, urea, or proteinuria prevalence. Inflammatory markers were mildly elevated and comparable between groups, consistent with chronic kidney disease related inflammation. SF-36 scores were broadly similar; post-COVID patients reported lower vitality (fatigue) but slightly better social functioning. Within the post-COVID cohort, multivariate logistic regression identified three independent predictors of advanced chronic kidney disease: proteinuria (adjusted OR 5.0; 95% CI 2.0–12.5; p<0.001), serum phosphate (OR 1.8 per +1 mg/dL; 95% CI 1.3–2.5; p<0.001), and hemoglobin (OR 1.4 per −1 g/dL; 95% CI 1.1–1.8; p=0.005). Model performance was strong (Hosmer–Lemeshow p=0.45; AUC ≈0.88).
Conclusions. COVID-19 history did not uniformly worsen medium-term renal outcomes in chronic kidney disease patients compared with matched non-COVID controls. However, persistent proteinuria, hyperphosphatemia, and anemia independently identified post-COVID patients at higher risk of advanced chronic kidney disease, supporting intensified post-COVID nephrology follow-up focused on these markers.
COVID-19, caused by SARS-CoV-2, is a multisystem disease with significant renal involvement. Acute kidney injury (AKI) develops in approximately 30% of hospitalized COVID-19 patients and in up to 50% of those admitted to intensive care units (ICU). In parallel, chronic kidney disease (CKD) represents a global “silent epidemic” and a leading contributor to morbidity and mortality worldwide [1]. The coexistence of COVID-19 and CKD therefore constitutes a syndemic condition, as CKD predisposes patients to severe COVID-19, while SARS-CoV-2 infection may induce direct and indirect renal injury through viral tropism for ACE2-expressing renal cells, systemic inflammation, ischemia, and microvascular dysfunction, potentially accelerating CKD progression [1, 2].
Growing observational evidence indicates that COVID-19 survivors face an increased risk of long-term renal complications [2, 3]. Large cohort studies have shown higher rates of kidney function decline, incident CKD, and progression to end-stage renal disease (ESRD) after COVID-19 compared with non-infected populations. Analysis of different data demonstrated a 15% increased risk of new or progressive CKD and more than a twofold increase in ESRD risk among COVID-19 survivors, including non-hospitalized cases [3, 4]. Patients requiring hospitalization or intensive care had markedly higher risks of adverse renal outcomes, with ICU-treated survivors exhibiting 7-13-fold higher odds of AKI, CKD progression, or dialysis dependence [5]. These findings highlight post-COVID renal impairment as a key component of long COVID syndrome [5-7]. Moreover, population-based data from Sweden confirmed a faster long-term decline in estimated glomerular filtration rate (eGFR) after COVID-19 compared with other pneumonias, particularly among hospitalized patients [8].
Despite this growing body of evidence, most studies originate from North America, Western Europe, or Asia, while data from Eastern Europe remain scarce [8]. In addition, available research has largely focused on general or acute COVID-19 cohorts, with limited attention to patients with pre-existing CKD [8, 9]. Consequently, the medium- and long-term renal trajectory of CKD patients after COVID-19, as well as the determinants of unfavorable progression, remain insufficiently characterized [10].
In this context, we conducted an original study in an Eastern European CKD cohort to evaluate post-COVID renal outcomes and to identify independent unfavorable prognostic factors for CKD progression using multivariate regression models. By comparing CKD patients with and without prior COVID-19 and integrating clinical, laboratory, and quality-of-life data, our study aims to improve risk stratification and inform targeted post-COVID follow-up strategies in this vulnerable population.
Study design and population
This research was designed as a prospective, observational cohort study with a parallel-group comparative approach. The study enrolled adult patients with pre-dialysis CKD (stages G1-G5 by KDIGO classification) under regular follow-up at a tertiary nephrology center in Chișinău, Moldova. Recruitment occurred during the post-pandemic period (2023-2024), once patients had recovered from acute COVID-19 if applicable. The cohort was split into two groups: a post-COVID-19 CKD group (exposed group) and a non-COVID CKD group (control group), each comprising 140 patients (total N=280). All patients gave informed consent to participate, and the study protocol was approved by the institutional ethics committee (favorable opinion of the Committee for Research Ethics at no.6 of 18.05.2023). Key inclusion and exclusion criteria were as follows:
Inclusion criteria: Age 18–70 years; Established CKD (stage G1–G5 pre-dialysis), either due to known chronic kidney disease or newly discovered eGFR <60 mL/min/1.73 m2 lasting >3 months; For the post-COVID group: a documented SARS-CoV-2 infection (positive PCR and/or serology) at least 1–3 months prior, with clinical recovery from acute illness; For the control group: no history of COVID-19 (no positive test or clinical diagnosis); Ability to provide informed consent and participate in follow-up evaluations.
Exclusion criteria: Age <18 or >70 years; End-stage kidney disease on dialysis or with a functioning kidney transplant; Active malignancy or tuberculosis (due to potential impacts on inflammation and survival); Any acute severe illness or decompensated condition at enrollment that could independently affect renal function (e.g. acute heart failure, sepsis); Immunosuppressive therapy for glomerulonephritis or other conditions (to avoid confounding effects on outcomes); Lack of consent or inability to comply with study procedures.
Patients meeting criteria were selected consecutively from clinic records and the hospital’s CKD registry, ensuring that the final sample reflected the real-world CKD population in our region. The two groups were frequency-matched on key variables (age, sex distribution, major comorbidities, and CKD stage/etiology) at baseline so that any differences observed could be attributed more confidently to the exposure (COVID-19) rather than underlying population differences.
Clinical data and measurements
All patients were evaluated using a standardized protocol at a post-COVID follow-up visit (exposed group) or an equivalent routine visit (controls). Data collection included medical history review, physical examination, laboratory investigations, and patient-reported outcomes. Recorded variables comprised demographics (age, sex), CKD characteristics (etiology, stage, duration), and major comorbidities (hypertension, diabetes mellitus, cardiovascular disease, obesity). In the post-COVID group, details of the SARS-CoV-2 infection were documented, including clinical severity (mild, moderate, severe), pulmonary involvement on chest CT, treatments received, and occurrence of acute kidney injury (AKI). AKI was defined according to KDIGO criteria (≥50% increase in serum creatinine or need for dialysis).
Laboratory assessments were performed in the same certified hospital laboratory. Renal function was evaluated by serum creatinine, urea, and estimated glomerular filtration rate (eGFR), calculated using the CKD-EPI 2021 equation. Urinalysis included dipstick and microscopy for proteinuria, hematuria, and leukocyturia; proteinuria was quantified by spot protein/creatinine ratio or 24-hour urinary protein excretion when indicated. Clinically significant proteinuria was defined as >0.3 g/24h or protein/creatinine ratio >0.3.
Inflammatory markers included erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), ferritin, and lactate dehydrogenase (LDH). Hematological evaluation comprised hemoglobin, leukocyte, and platelet counts; anemia was defined using WHO criteria. Additional biochemical parameters relevant to CKD were measured, including serum albumin, electrolytes, calcium, phosphate, liver enzymes, fasting glucose, HbA1c, and lipid profile. In post-COVID patients, D-dimer levels were assessed as a marker of residual hypercoagulability. All samples were collected under fasting conditions.
Health-related quality of life was assessed using the validated Short Form-36 (SF-36) questionnaire, covering physical and mental health domains. Scores were compared between groups to evaluate the impact of COVID-19 on patient-perceived health status.
Follow-up and outcome definition
Analyses were based on a single cross-sectional follow-up, performed at a median of approximately 6 months after COVID-19 recovery. The primary outcome was unfavorable CKD progression, defined as advanced CKD stage (G4-G5) at follow-up, compared with stages G1-G3. Secondary outcomes included significant decline in eGFR (>25% from estimated pre-COVID baseline, where available), persistence or worsening of abnormal urinalysis, and changes in CKD-related extrarenal complications.
Statistical analysis
Statistical analyses were performed using STATISTICA v.10.0. Continuous variables were expressed as mean ± standard deviation or median [interquartile range], and categorical variables as frequencies and percentages. Group comparisons used Student’s t-test or Mann-Whitney U test for continuous data and Chi-square or Fisher’s exact test for categorical data; correlations were assessed using Pearson or Spearman coefficients, as appropriate. Multivariate logistic regression was applied to identify independent prognostic factors for CKD progression in post-COVID patients, with advanced CKD stage (G4-G5) as the dependent variable. Candidate predictors included demographic and CKD-related variables, comorbidities, proteinuria, serum phosphate, hemoglobin, inflammatory markers, D-dimer, and COVID-19 severity or AKI. A backward stepwise approach retained variables with p<0.1. Results are reported as adjusted odds ratios (OR) with 95% confidence intervals. Model performance was evaluated using the Hosmer-Lemeshow test and area under the ROC curve (AUC). Missing data were minimal (<5%) and handled by case-wise deletion.
Patient Characteristics
A total of 280 CKD patients were included, comprising 140 post-COVID patients and 140 non-COVID controls (Table 1). The groups were well matched for age (mean 53.4 ± 12.6 years; p=0.72) and sex (52% vs 49% male; p=0.68). The prevalence of major comorbidities was similar, including hypertension (~85% in both groups), obesity (~28% vs 25%), and cardiovascular disease (~20% each; all p>0.2). Diabetes mellitus was more frequent in the post-COVID group (31.4% vs 21.4%), showing a borderline difference (p≈0.058).
| Characteristic | Post-COVID CKD (n = 140) |
Non-COVID CKD (n = 140) |
p value |
|---|---|---|---|
| Age, years (mean ± SD) | 53.6 ± 12.4 | 53.2 ± 12.8 | 0.72 |
| Male sex, n (%) | 73 (52.1) | 69 (49.3) | 0.68 |
| Duration of CKD, years (median) | 4.6 | 4.5 | 0.84 |
| Hypertension, n (%) | 119 (85.0) | 118 (84.3) | 0.88 |
| Diabetes mellitus, n (%) | 44 (31.4) | 30 (21.4) | 0.058 |
| Obesity, n (%) | 39 (27.9) | 35 (25.0) | 0.60 |
| Cardiovascular disease, n (%) | 29 (20.7) | 27 (19.3) | 0.77 |
| CKD etiology, n (%) | |||
| - Chronic glomerulonephritis | 58 (41.4) | 60 (42.9) | 0.79 |
| - Diabetic nephropathy | 25 (17.9) | 21 (15.0) | 0.50 |
| - Hypertensive nephropathy | 34 (24.3) | 36 (25.7) | 0.78 |
| - Other etiologies | 23 (16.4) | 23 (16.4) | 1.00 |
| Baseline CKD stage, n (%) | |||
| - G1-G3a | 32 (22.9) | 32 (22.9) | 1.00 |
| - G3b | 31 (22.1) | 31 (22.1) | 1.00 |
| - G4 | 42 (30.0) | 42 (30.0) | 1.00 |
| - G5 (pre-dialysis) | 35 (25.0) | 35 (25.0) | 1.00 |
Note: CKD - chronic kidney disease; SD - standard deviation. Baseline demographic characteristics, comorbidities, CKD etiology, and CKD stage distribution were comparable between post-COVID and non-COVID CKD groups, ensuring balanced baseline risk profiles.
The distribution of CKD etiologies was comparable, with chronic glomerulonephritis and diabetic nephropathy predominating in both cohorts. Median CKD duration was similar (≈4.5 years; p=0.84). By design, baseline CKD stages were matched: 22% G3b, 30% G4, and 25% G5 in each group, ensuring comparable baseline renal risk profiles.
COVID-19 episode details
Among post-COVID patients, 60% experienced moderate disease, 25% severe disease, and 15% mild outpatient-managed infection. The median interval from recovery to evaluation was 6 months (IQR 4-8). COVID-associated AKI occurred in 18 patients (12.9%), mostly KDIGO stage 1–2, with renal function recovery in all but one case. Persistent respiratory symptoms were reported by 20% of patients, while none required long-term oxygen therapy. These variables were descriptively analyzed and not included in the primary renal outcome models.
Comparative clinical outcomes: post-COVID vs non-COVID CKD
At follow-up, renal function did not differ significantly between groups. Mean serum creatinine (157 ± 140 vs 168 ± 152 µmol/L; p=0.53), blood urea (10.30 ± 7.23 vs 10.46 ± 6.97 mmol/L; p=0.85), and eGFR (~35 mL/min/1.73m2 in both; p=0.79) were comparable. The prevalence of proteinuria was similarly high (51% vs 48%), with no differences in median protein excretion or nephrotic-range proteinuria. Hematuria and leukocyturia occurred in approximately half of patients in both groups, reflecting underlying CKD etiologies.
Inflammatory markers were comparable between groups, including CRP (6.1 vs 5.5 mg/L; p=0.40), ESR (23 vs 24 mm/h; p=0.51), and ferritin (median ~250 µg/L; p=0.88). No evidence of persistent systemic inflammation or hypercoagulability was observed; D-dimer levels were normalized and similar between groups (p=0.58), and no late thromboembolic events were recorded.
Hematologic parameters were likewise unaffected by past COVID. Both groups exhibited the mild-to-moderate normocytic anemia typical of CKD; mean hemoglobin was 10.8 g/dL in post-COVID vs 11.0 g/dL in controls (p = 0.45), with anemia prevalence ~85% in each group. No differences were seen in total white cell or platelet counts. These results confirm that COVID-19 did not significantly exacerbate or alter the hematologic profile of CKD patients in the medium term. For example, the degree of anemia and occasional leukopenia were similar and attributable to CKD itself rather than any post-viral effect.
Metabolic factors showed minimal differences between groups. Serum albumin was slightly lower in post-COVID patients than in controls (38.0 ± 5.1 vs 39.5 ± 4.8 g/L, p=0.04), but values remained within the normal range, indicating preserved nutritional status. Fasting glucose was modestly higher in the post-COVID group (6.4 vs 5.9 mmol/L, p=0.048), whereas HbA1c levels were similar (p=0.77), suggesting no significant long-term deterioration of glycemic control. Lipid profiles and liver function tests did not differ between groups, indicating recovery of metabolic and hepatic homeostasis by approximately 6 months after infection.
Cardiopulmonary status revealed subtle cardiovascular differences. A higher proportion of post-COVID patients had symptomatic heart failure, with NYHA class III observed in 12% versus 5% of controls, and fewer post-COVID patients being asymptomatic. Blood pressure control was comparable between groups. Cardiac arrhythmias were less frequent in post-COVID patients (10% vs 18%, p=0.08). No persistent respiratory impairment was identified: pulmonary examination, oxygen saturation, and follow-up imaging showed no evidence of chronic lung damage. Overall, COVID-19 survivors demonstrated a tendency toward more advanced heart failure, while respiratory recovery was complete and similar to controls.
Quality of life (QoL) assessment using SF-36 showed no significant differences in overall scores or most domains. Physical and mental component summary scores were comparable between groups. However, post-COVID patients reported lower vitality scores (greater fatigue; p<0.05), consistent with post-COVID fatigue, and slightly higher social functioning (p=0.04). Other domains, including role physical and role emotional, were similar. Self-rated health compared with the previous year did not differ between groups.
Overall, a resolved COVID-19 episode was not associated with sustained multisystem deterioration or accelerated renal decline at the cohort level. Post-COVID and non-COVID CKD patients followed similar medium-term clinical trajectories, largely determined by baseline CKD severity and comorbidities. These findings suggest that most CKD patients can recover their pre-COVID clinical status, although a subset remains at risk for adverse renal outcomes, as explored in subsequent analyses.
Prognostic factors for CKD progression in post-COVID patients
Despite the generally favorable average outcomes noted above, there was variability within the post-COVID CKD group in terms of renal disease trajectory. Some patients remained stable or even had slight improvements in eGFR (perhaps due to optimized care post-COVID), whereas others progressed to more advanced CKD stages faster than expected. To discern what baseline or post-infection factors might explain these divergent paths, we performed multivariate regression analyses focusing on the post-COVID cohort.
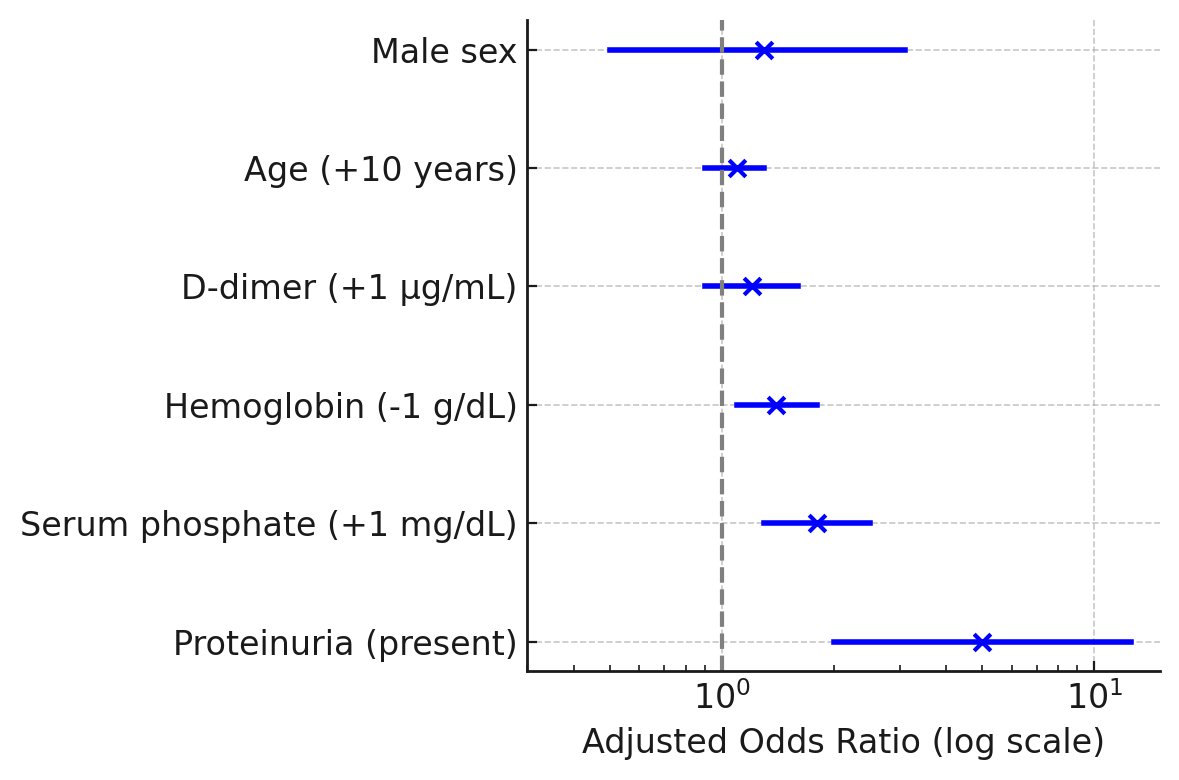
Multivariate logistic regression identified three independent prognostic factors for unfavorable renal outcome (advanced CKD stage G4-G5) in post-COVID patients: proteinuria, hyperphosphatemia, and anemia (Figure 1). Proteinuria was the strongest predictor; patients with significant proteinuria had a fivefold higher likelihood of advanced CKD (adjusted OR 5.0, 95% CI 2.0-12.5, p<0.001). Serum phosphate was the second strongest predictor, with each 1 mg/dL increase associated with an ~80% increase in risk (OR 1.8, 95% CI 1.3-2.5, p<0.001). Hemoglobin showed an inverse association: each 1 g/dL decrease increased the odds of advanced CKD by 40% (OR 1.4, 95% CI 1.1-1.8, p=0.005). All three variables remained independently significant, indicating complementary prognostic value.
Other variables were not retained in the adjusted model. D-dimer showed a non-significant trend (OR ~1.2 per +1 μg/mL, 95% CI 0.9–1.6, p=0.10). Age (OR ~1.1 per decade, p=0.18), male sex (OR ~1.3, p=0.60), diabetes mellitus, and uncontrolled hypertension lost significance after adjustment, likely because their effects were mediated through proteinuria and CKD severity.
Model performance was robust, with good calibration (Hosmer-Lemeshow χ2=7.1, p=0.45) and excellent discrimination (AUC ≈0.88). ROC analysis showed AUC values of ~0.75 for proteinuria, ~0.78 for serum phosphate (optimal cutoff ≈5.0 mg/dL; sensitivity ~70%, specificity ~75%), and ~0.70 for hemoglobin (cutoff ≈10 g/dL).
Subgroup analysis showed a higher prevalence of advanced CKD among patients with severe COVID-19 compared to mild/moderate disease (70% vs 45%, p=0.01); however, COVID-19 severity and post-COVID AKI were not independent predictors after adjustment (p=0.27), indicating mediation through CKD-related factors.
Risk stratification demonstrated that patients without any of the three risk factors had a low probability (~10%) of advanced CKD at 6 months, whereas the presence of all three conferred a very high risk (>90%). Patients with one or two factors represented an intermediate-risk group, highlighting the clinical utility of this model for targeted post-COVID CKD management.
In this study, we explored the relationship between COVID-19 and CKD progression in a cohort from an Eastern European tertiary center, providing complementary evidence to the growing literature on post-COVID organ damage. At the cohort level, CKD patients who recovered from COVID-19 did not demonstrate a uniform deterioration of renal function or persistent systemic sequelae in the medium term compared with matched CKD patients without COVID. This reassuring finding indicates that the average post-COVID CKD patient largely returned to the expected trajectory of chronic kidney disease. Specifically, we observed no significant differences in eGFR, proteinuria, or CKD-related complications, including anemia and mineral bone disorder parameters, attributable directly to COVID-19 several months after infection [11]. These results are consistent with reports showing that although COVID-19 can induce acute kidney injury, many patients – particularly those who survive non-critical disease – can recover near-baseline renal function after the acute phase. In our cohort, COVID-associated AKI was largely transient, as reflected by the absence of intergroup differences in serum creatinine at follow-up. Moreover, inflammatory and hypercoagulability markers (CRP, ESR, D-dimer) normalized, suggesting that COVID-related systemic inflammation had resolved and was unlikely to drive ongoing kidney injury at this stage.
At first glance, these findings may appear discordant with large epidemiological studies [11, 12], which reported increased risks of CKD progression and adverse renal outcomes among COVID-19 survivors. However, those analyses included heterogeneous populations, many without pre-existing CKD and with a higher proportion of critically ill patients. In contrast, our study focused exclusively on individuals with established CKD who survived COVID-19 [13, 14]. Within this more homogeneous population, outcomes were heterogeneous rather than uniformly adverse [13, 14]. The lack of an average difference between post-COVID and non-COVID CKD groups likely reflects this variability: while many patients followed their expected CKD trajectory, a vulnerable subset experienced accelerated progression [14]. Thus, our findings refine rather than contradict large-scale observations by highlighting that excess renal risk after COVID-19 is concentrated in specific high-risk subgroups.
Using multivariate regression, we demonstrated that the principal drivers of CKD progression after COVID-19 were classical CKD-related factors – proteinuria, hyperphosphatemia, and anemia – rather than COVID-specific variables. This supports the concept that COVID-19 primarily exacerbates underlying CKD pathology in susceptible patients rather than introducing novel mechanisms of chronic renal injury [15]. Proteinuria emerged as the strongest prognostic factor, with a fivefold increase in the odds of advanced CKD [15]. As a marker of ongoing glomerular damage and a mediator of tubulointerstitial injury, persistent proteinuria after COVID-19 should prompt intensified renoprotective therapy. This observation aligns with recent reports emphasizing the prognostic significance of persistent proteinuria in COVID survivors.
Hyperphosphatemia was the second independent predictor, consistent with its known associations with reduced GFR, secondary hyperparathyroidism, vascular calcification, and renal fibrosis [16]. Poor phosphate control may reflect advanced CKD, treatment non-adherence, or care disruption during acute illness. Regardless of mechanism, our findings reinforce the importance of monitoring and managing mineral metabolism disturbances in post-COVID CKD patients, as suggested by interventional studies linking phosphate reduction to slower CKD progression [17].
Anemia also independently predicted adverse outcomes, with lower hemoglobin levels associated with higher risk of advanced CKD. Anemia in post-COVID CKD patients is likely multifactorial, reflecting disease severity and possibly residual inflammatory or marrow effects, and contributes to renal hypoxia and progression [17, 18]. This finding is consistent with prior studies linking anemia severity to accelerated CKD decline and highlights the need for optimized anemia management in post-COVID care [17, 18].
Importantly, acute COVID-19 severity and related variables did not retain independent prognostic significance after adjustment for CKD-related factors [19, 20]. Although severe COVID-19 was associated with a higher prevalence of advanced CKD on univariate analysis, its effect appeared to be mediated through AKI and worsening CKD markers rather than acting independently. This interpretation is supported by previous follow-up studies, including data from China and Sweden, demonstrating that long-term renal risk is most pronounced in patients with AKI or severe pneumonia, whereas mild COVID-19 without renal involvement has limited long-term impact after accounting for baseline kidney status [20, 21].
Clinically, these findings support a risk-stratified approach to post-COVID CKD follow-up. Comprehensive renal assessment – including eGFR, proteinuria, and phosphate evaluation – should be performed several months after recovery, particularly in high-risk patients [20, 21]. Intensification of standard CKD therapies (RAAS blockade, phosphate control, anemia correction) appears essential to mitigate progression. From a health system perspective, identifying patients at highest risk allows efficient allocation of nephrology resources, especially in settings with limited dialysis capacity.
Quality-of-life outcomes provide additional reassurance: despite persistent fatigue, post-COVID CKD patients reported social and emotional well-being comparable to controls, suggesting resilience and recovery beyond biological parameters [22, 23]. Nevertheless, fatigue should be addressed as a distinct component of post-COVID care.
Several limitations warrant consideration, including the relatively short follow-up, cross-sectional assessment of CKD progression, single-center design, and limited sample size for regression analyses. Unmeasured confounders and lack of detailed inflammatory or histopathological markers may also have influenced results. However, the controlled design, focus on an underrepresented Eastern European CKD population, and comprehensive clinical assessment strengthen the validity and relevance of our findings.
In summary, our study conveys a cautiously optimistic message: CKD patients can recover from COVID-19 without uniform renal deterioration, but a vulnerable subgroup – characterized by proteinuria, hyperphosphatemia, and anemia – remains at high risk for progression. Early identification and targeted management of these factors are crucial to preventing end-stage kidney disease in the post-COVID era.
In this original study of CKD patients in the post-COVID era, we found that an episode of COVID-19 did not inevitably accelerate CKD progression for all patients; many recovered to their pre-infection baseline. However, certain unfavorable prognostic factors clearly delineate which patients are at risk for worsening renal function. Persistent proteinuria, elevated serum phosphate, and low hemoglobin levels were identified as independent predictors of advanced CKD progression after COVID-19. These factors appear to capture the residual kidney injury and aggravated CKD milieu induced by the infection. Patients with any of these risk markers should be considered a high-risk subgroup for whom closer monitoring and aggressive CKD management are warranted. Conversely, absence of proteinuria and good control of metabolic parameters portend a more benign course even after COVID-19.
In practical terms, our conclusions are: (1) Post-COVID CKD follow-up is essential – clinicians should evaluate proteinuria, GFR, and CKD complications in all CKD patients who had COVID-19, approximately 3-6 months after recovery, to stratify risk. (2) Proteinuria is the red flag – its presence signals active disease and need for interventions (RAAS blockade, etc.), whereas its absence is reassuring. (3) Manage what is manageable – treat anemia and hyperphosphatemia diligently in post-COVID CKD patients, as these not only reflect disease severity but could also exacerbate progression. (4) Personalized monitoring – patients with multiple risk factors may need expedited preparation for renal replacement therapy or inclusion in interventional trials, whereas those without may follow standard CKD care. (5) Holistic care – beyond numbers, address symptoms like fatigue in post-COVID patients to improve quality of life, as overall QoL can remain good with supportive care.
The authors thank all the patients who participated in this study and the clinical staff of the Nephrology Department at „Timofei Moșneaga” Clinical Republican Hospital for their invaluable assistance with patient recruitment and data collection, for advice on study design and to the laboratory personnel for ensuring high-quality assays. We are also grateful to entire medical team, who stood at the forefront of the fight against COVID-19. Their professionalism, dedication and unwavering commitment during the most challenging phases of the pandemic were essential in ensuring high-quality patient care under unprecedent conditions. The authors particularly acknowledge the collective effort, resilience and solidarity of physicians, nurses and allied healthcare professionals, whose tireless work and human compassion made this research possible and contributed profoundly to the care of patients included in this study.
Al-Aly Z, Xie Y, Bowe B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature. 2021;594(7862):259-264. doi:10.1038/s41586-021-03553-9
Akilesh S, Nast CC, Yamashita M, et al. Multicenter Clinicopathologic Correlation of Kidney Biopsies Performed in COVID-19 Patients Presenting With Acute Kidney Injury or Proteinuria. Am J Kidney Dis. 2021;77(1):82-93.e1. doi:10.1053/j.ajkd.2020.10.001
Al-Aly Z, Agarwal A, Alwan N, Luyckx VA. Long COVID: long-term health outcomes and implications for policy and research. Nat Rev Nephrol. 2023 Jan;19(1):1-2. doi: 10.1038/s41581-022-00652-2.
Al-Aly Z, Bowe B, Xie Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med. 2022;28(7):1461-1467. doi:10.1038/s41591-022-01840-0
Birkelo BC, Parr SK, Perkins AM, et al. Comparison of COVID-19 versus influenza on the incidence, features, and recovery from acute kidney injury in hospitalized United States Veterans. Kidney Int. 2021;100(4):894-905. doi:10.1016/j.kint.2021.05.029
Henry BM, Lippi G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int Urol Nephrol. 2020;52(6):1193-1194. doi:10.1007/s11255-020-02451-9
Legrand M, Bell S, Forni L, et al. Pathophysiology of COVID-19-associated acute kidney injury. Nat Rev Nephrol. 2021;17(11):751-764. doi:10.1038/s41581-021-00452-0
Tran VT, Porcher R, Pane I, Ravaud P. Course of post COVID-19 disease symptoms over time in the ComPaRe long COVID prospective e-cohort. Nat Commun. 2022;13(1):1812. Published 2022 Apr 5. doi:10.1038/s41467-022-29513-z
Jana KR, Yap E, Janga KC, Greenberg S. Comparison of Two Waves of COVID-19 in Critically Ill Patients: A Retrospective Observational Study. Int J Nephrol. 2022;2022:3773625. doi:10.1155/2022/3773625
Bowe B, Xie Y, Xu E, Al-Aly Z. Kidney Outcomes in Long COVID. J Am Soc Nephrol. 2021;32(11):2851-2862. doi:10.1681/ASN.2021060734
Liakopoulos V, Roumeliotis S, Papachristou S, Papanas N. COVID-19 and the kidney: time to take a closer look. Int Urol Nephrol. 2022;54(5):1053-1057. doi:10.1007/s11255-021-02976-7
Jewell PD, Bramham K, Galloway J, et al. COVID-19-related acute kidney injury; incidence, risk factors and outcomes in a large UK cohort. BMC Nephrol. 2021;22(1):359. doi:10.1186/s12882-021-02557-x
Răzlog T, Russu E, Ceban E, Groza C, Alexa Z, Groppa L. Factorii de progresie ai bolii cronice de rinichi la pacienții cu COVID-19. Revista de Ştiinţe ale Sănătăţii din Moldova. 2024;11(2 suppl):59.
Răzlog T, Russu E, Alexa Z, Ceban E, Groza C, Groppa L. Manifestations of kidney involvement in COVID-19 patients and progression to chronic kidney disease. Revista de Ştiinţe ale Sănătăţii din Moldova. 2024;11(1):11-18. doi:10.52645/MJHS.2024.1.02
Chaudhri I, Moffitt R, Taub E, et al. Association of Proteinuria and Hematuria with Acute Kidney Injury and Mortality in Hospitalized Patients with COVID-19. Kidney Blood Press Res. 2020;45(6):1018-1032. doi:10.1159/000511946
Chu CD, McCulloch CE, Banerjee T, et al. CKD Awareness Among US Adults by Future Risk of Kidney Failure. Am J Kidney Dis. 2020;76(2):174-183. doi:10.1053/j.ajkd.2020.01.007
Coresh J, Byrd-Holt D, Astor BC, et al. Chronic kidney disease awareness, prevalence, and trends among U.S. adults, 1999 to 2000. J Am Soc Nephrol. 2005;16(1):180-188. doi:10.1681/ASN.2004070539
Couchoud C, Bayer F, Ayav C, et al. Low incidence of SARS-CoV-2, risk factors of mortality and the course of illness in the French national cohort of dialysis patients. Kidney Int. 2020;98(6):1519-1529. doi:10.1016/j.kint.2020.07.042
Eligulashvili A, Gordon M, Lee JS, et al. Long-term outcomes of hospitalized patients with SARS-CoV-2/COVID-19 with and without neurological involvement: 3-year follow-up assessment. PLoS Med. 2024;21(4):e1004263. Published 2024 Apr 4. doi:10.1371/journal.pmed.1004263
Farouk SS, Fiaccadori E, Cravedi P, Campbell KN. COVID-19 and the kidney: what we think we know so far and what we don't. J Nephrol. 2020;33(6):1213-1218. doi:10.1007/s40620-020-00789-y
Fisher M, Neugarten J, Bellin E, et al. AKI in Hospitalized Patients with and without COVID-19: A Comparison Study. J Am Soc Nephrol. 2020;31(9):2145-2157. doi:10.1681/ASN.2020040509
Graham EL, Clark JR, Orban ZS, et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized Covid-19 "long haulers". Ann Clin Transl Neurol. 2021;8(5):1073-1085. doi:10.1002/acn3.51350
Havervall S, Rosell A, Phillipson M, et al. Symptoms and Functional Impairment Assessed 8 Months After Mild COVID-19 Among Health Care Workers. JAMA. 2021;325(19):2015-2016. doi:10.1001/jama.2021.5612